By Sara Rubin, MPH, MA, Senior Program Analyst, Pandemic and Catastrophic Preparedness, NACCHO and Alyson Jordan, MPA, Communications Specialist, Public Health Preparedness, NACCHO
Since 2007, continued funding cuts have been impacting pandemic influenza planning and response in local health departments (LHDs). Sequestration, the automatic federal spending cuts that took place in March 2013, caused further strain on these programs. With another round of sequestration cuts set to take place in January 2014, LHDs may be forced to reduce or eliminate programs that would plan for and respond to a pandemic influenza outbreak. Should a strain of severe influenza—such as the H7N9 virus that emerged earlier this year in China—spread across the United States, many local health departments could be limited by budget constraints and not fully equipped to respond.
 As LHDs are looking ahead to the next fiscal year and anticipating more funding cuts, these examples of the consequences of past funding cuts may provide insight into what LHDs should prepare for if planned sequestration cuts move forward:
As LHDs are looking ahead to the next fiscal year and anticipating more funding cuts, these examples of the consequences of past funding cuts may provide insight into what LHDs should prepare for if planned sequestration cuts move forward:
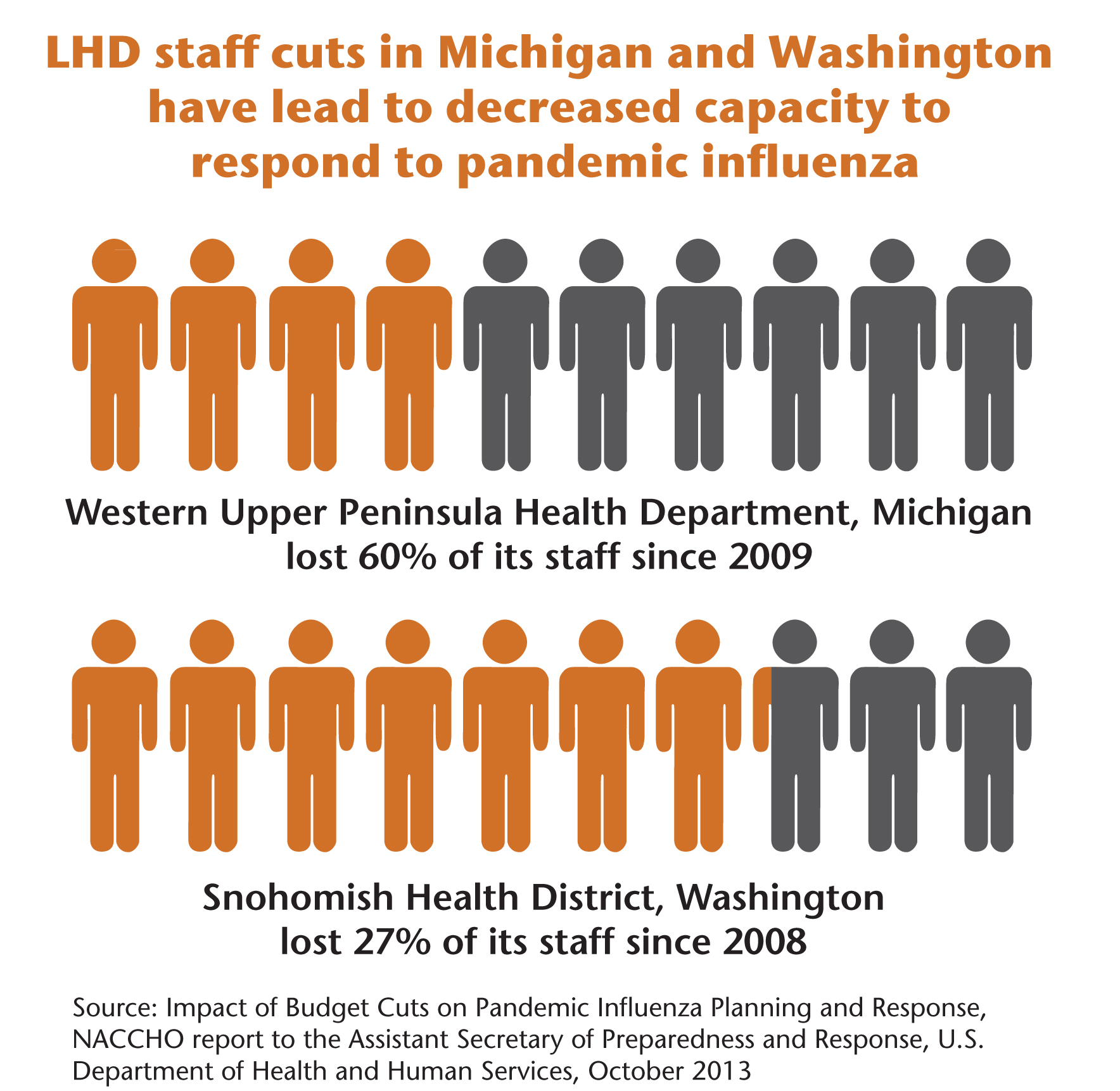
- Western Upper Peninsula Health Department, Michigan has seen its staffing drop from 112 to 45 since 2009, a 60 percent reduction due to program losses, a changing healthcare market, and declining revenue sources. The LHD serves the northernmost and westernmost reaches of the state, with 70,000 residents scattered across 5,000 rugged square miles. These budget cuts and subsequent staff reductions have made it difficult for the health department to fill each crucial emergency response role with at least one staff member. The shift in planning for public health emergencies, including influenza pandemics, has moved from doing more with less, to doing less with less because the needed resources are not available.
- Ramsey County, Minnesota eliminated the health educator position that reached out to its 100 percent urbanized and highly diverse community after cuts in pandemic preparedness funding. Racial and ethnic minorities comprise over a third of the population of over a half million residents. In addition, the cuts severely limit the ability to produce influenza risk communication materials in the most prevalent languages in Ramsey County, as well as in low-literacy English. During the H1N1 pandemic in 2009, the health educator accomplished significant outreach to their Limited English Proficiency (LEP) and refugee populations, which are mostly uninsured or underinsured, and distributed thousands of flyers on the risk of flu. This targeted outreach resulted in the majority of the thousands of clients at H1N1 mass vaccination clinics to be LEP residents. For example, busloads of recently arrived refugees from Burma came to their mass vaccination clinics directly due to funded outreach to LEP community members.
- Douglas and Cobb County Health Department, Georgia reduced its critical disaster response staff after significant budget cuts. After H1N1, budget cuts brought a full time emergency preparedness risk communication position from full-time to part-time (50 percent). Now, the current year budget cut has caused them to eliminate that position entirely. This staffing cut could prove to be extremely problematic in the face of another pandemic because no staff would be able to immediately deal with developing critical messages for the public, the media, medical care providers, and hospitals. Due to past experiences with daily changes in Centers for Disease Control and Prevention public guidance, strong risk communications skills are vital, and the loss is extremely difficult to overcome.
- Snohomish Health District, Washington cut its workforce by 27 percent over 2008-2009. As a result, the district has reduced capacity to respond to public health disasters. For H1N1, Snohomish County was able to build a coalition of health department staff, community volunteers, and public and private sector partners to support 20 vaccination clinics during the influenza pandemic. However, sequestration cuts could compromise that coalition. An eight percent reduction in federal funding equates to $240,000 in losses to this health department ($62,000 in preparedness alone), staff cuts to their four-person preparedness team, and even more lost capacity for coalition building.
While these examples provide insights into the consequences of funding cuts in specific LHDs, reductions in preparedness programs reflect a national trend identified in NACCHO’s 2013 Job Losses and Program Cuts survey. This comprehensive snapshot of the state of the nation’s local health departments was administered in early 2013 before the sequestration cuts took effect, and analyzed the impacts of budget, staffing, and program cuts in 2012. At a national level, LHDs collectively lost 43,900 jobs since 2008. Among other programmatic cuts, 23 percent of LHDs reduced or eliminated emergency preparedness programs in 2011, and the trend continued in 2012 with 15 percent of LHDs reporting a reduction in emergency preparedness programs. If sequestration persists, LHDs can expect more funding cuts that will have an effect on their preparedness and other public health programming.
Has your LHD been impacted by budget cuts? Let us know how your LHD has responded to budget cuts in the comment box below and learn how you can get involved.