Global-to-Local Public Health

Public health professionals around the world face many of the same challenges. While the United States is making bold strides in some areas of health, public health practitioners beyond our borders–even those with limited resources–have made significant progress in areas where we lag.
NACCHO’s Global Health Program explores how these successful approaches to public health in other countries can be adopted and adapted by local health departments to promote the health and well-being of all Americans. Ultimately, the health and well-being of all people are intrinsically related and may be approached with similar solutions.
NACCHO will provide guidance to encourage local health departments to
adopt new strategies and learn from communities that, at first glance,
may not look like their own.
“Global health innovations can offer unique perspective on ways to improve health outcomes through novel, creative approaches. Local health departments can learn from and adapt these innovations to improve health within their communities.”
– Lori Tremmel Freeman, CEO, NACCHO
Given the health system differences between a global approach’s country of origin and the United States, some adaptation will be needed to ensure it is appropriate in a new context. This can be a challenge for local health departments (LHDs), and discussions with health department leaders have indicated that uncertainty about this process can be a barrier to adopting global health approaches. Therefore, NACCHO has developed the below guidance on the most effective strategies for LHDs to adapt global health solutions so that the entire globe can be a resource for new solutions to challenging problems.
Take note that this is a living document that will be regularly updated as more information becomes available!
How to use this guide
This guide is meant to assist LHDs through the thought process surrounding the adoption and adaptation of a global approach. We have broken down the guidance into three general steps:
- Assessing the elements to adapt: Determining what elements of the global approach you can change without corrupting the effectiveness of the program
- Adapting the appropriate elements of an approach: Changing only the parts that will make the approach more effective in your community
- Diffusing the approach into your community and communicating it effectively: How to tailor diffusion to different groups and share the benefits while addressing people’s concerns
* Important to Note: Much of the information in this guidance comes from general research on adapting approaches from different communities or cultures and not specifically a global approach into the United States. NACCHO is actively collecting information related to adopting and adapting global health programs to U.S. LHDs specifically, and that information will be compiled for version 2 (v.2).
Assessing the Elements to Adapt
- Cultural adaptation: Tailoring the intervention to meet the community’s worldview and lifestyle
- Cognitive adaptation: Changing the language, reading, or age level of the intervention
- Environmental adaptation: Ecological aspects of the community, for example implementing in homes instead of at a clinic
- Program content adaptation: Tailoring of language, visuals, examples, scenarios, and activities used during the intervention
- Program form adaptation: Altering program structure and goals, which have a potential to reduce program effectiveness
Adaptations
| Green Light | Yellow Light | Red Light |
|---|---|---|
| GO! These are changes to ensure a better fit for the culture or context of the population • Updating and/or customizing statistics or information as it is relevant to the community • Making activities more interactive, appealing to different learning styles |
CAUTION! These are changes that can be made, but in a way that ensure the core components are adhered to • Changing session order or sequence of activities • Adding activities to reinforce learning or to address additional risk and protective factors • Implementing program with a different population or in a different setting |
STOP! These remove or alter key aspects that can weaken the original program’s effectiveness • Shortening a program • Reducing or eliminating activities • Contradicting, competing with, or diluting the program’s goals |
Adapting the Appropriate Elements of an Approach
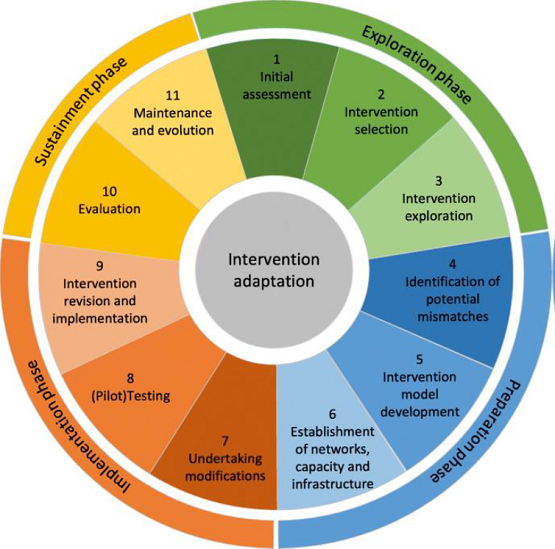
Adapting evidence-informed complex population health interventions for new contexts: a systematic review of guidance provided this intervention adaptation wheel as a visual for the steps that an LHD would go through when adapting an approach.
Consider these as your basic steps for effective adaptation. While all may not be necessary for each individual circumstance, each are important and should be considered as you go through the process of adapting a global approach to address the needs of your local community.
| Step | Description |
|---|---|
| 1. Assess community | - Identify needs of target population - Assess organizational capacity to implement the program |
| 2. Understand the intervention | - Understand the theory behind the programs and their core elements |
| 3. Consult with experts | - Incorporate expert advice into program |
| 4. Consult with stakeholders | - Seek input from advisory boards and community planning groups where program implementation takes place |
| 5. Identify potential mismatches and decide what needs adaptation | - Identify and categorize potential mismatches (e.g., among intervention goals, characteristics of the target population, implementation agency, and/or community) - Identify potential implementation barriers - Identify potential barriers to participation - Determine what core components are especially needed to maintain and address fidelity - Determine how original and new target population/setting differ in terms of risk and protective factors |
| 6. Adapt the original program | - Adapt the original program contents through collaborative efforts - Make adaptations continuously through pilot testing - Core components responsible for change should not be modified |
| 7. Train staff | - Select and train staff to ensure quality implementation |
| 8. Test the adapted materials | - Pretest adapted materials with stakeholder groups - Conduct readability tests - Modify approach further if necessary |
| 9. Implement | - Develop implementation plan based on results generated in previous steps - Develop scope, sequence, and instructions - Execute adapted approach |
| 10. Evaluate | - Document the adaptation process and evaluate the process and outcomes of the adapted intervention as implemented |
| 11. Maintenance and evolution | - Establish a wide-scale dissemination of the adapted intervention, given the intervention is successful and is embraced by the community - Develop training systems to widen the dissemination (e.g., train future implementers in the adapted version of the intervention) - Implement an ongoing re-assessment |
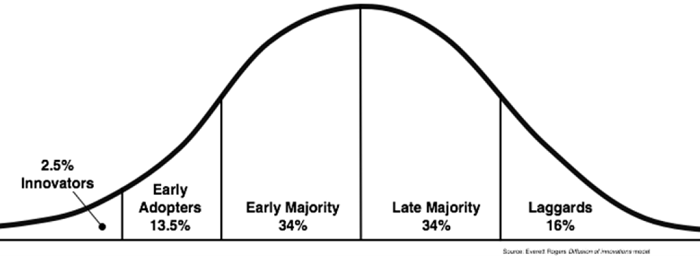
Diffusing the Approach into your Community and Communicating it Effectively
Once the intervention has been selected and adaptations have been made, it is time to diffuse the intervention throughout the community. The Diffusion of Innovation Theory was developed by E.M. Rogers in 1962 and is a cornerstone of social science theories. It explains the process that innovations go through after introduction, indicating the different categories of people who will ultimately adopt the new innovation. Each category in the curve has their own specific strategies for how to approach them most effectively to encourage innovation to the adopting of a new approach:
Additional Resources
Learn about global-to-local success stories here.
Featured Stories



Success Stories by Location
| Program | Description | Location |
|---|---|---|
| Bringing Global Health Home: The Case of Global to Local in King County, Washington | General overview of potential options for approaches that can be adapted from global health to be effective in local U.S. public health | King County, WA |
| CHW model from Venezuela to Orange County, California and back | A doctor from Venezuela recognizes the value of community health workers (CHWs) to improve health outcomes for the population in Orange County, California | Orange County, CA |
| Global vector control strategies in Harris Countyto prevent infectious mosquito-borne diseases | Approaches from Australia, India, Vietnam, Indonesia, China, Siri Lanka, Fiji, New Caledonia, Mexico, Brazil, and Columbia, provide inspiration for vector-control strategies to prevent Zika, Chikungunya, Dengue, West Nile virus,and Saint Louis encephalitis in Harris County, Texas | Harris County, TX |
| How Healthy is Your Main Street? Adapting an Approach from the United Kingdom | A British program to determine how healthy high streets are based on their storefronts is adapted to measure the health on U.S. main streets | Los Angeles, CA |
| Zimbabwe’s Friendship Benches in New York City | Zimbabwe placed benches in areas where mental health services were needed and trained grandmothers to provide basic mental health services. Now New York City is trying the same approach | New York City, NY |
| Cuban Maternity Care Policy Could Improve MMR and IMR in Rural Alabama | Improved prenatal care for women with high-risk pregnancies in Cuba adapted to address the needs of similar women in rural Alabama | Alabama |
Podcast Episodes
More global health-related episodes from NACCHO's podcast:
Read featured NACCHO articles and listen to related Podcast from Washington episodes.
