Health Disparities Disparate Impact
This page requires a membership login. Log in or create an account by clicking the link below.
MyNACCHO Login
Health disparities are Differences in health outcomes that are linked to inequities in social, economic, or environmental conditions.
- Encourage your LHD to commit to addressing health disparities before embarking on meaningful change. Think critically about what that commitment means. Health equity work requires organizational buy-in, resources, and support for innovation. When an LHD explicitly names health equity as a priority, efforts may be more likely to succeed. Organizational commitments can take many forms depending on what health equity efforts are already underway. For example, an LHD that is new to health equity work may first commit to gathering information to gain a better understanding of local health disparities, while another LHD that has already integrated health equity into a strategic plan may commit to launching a related program or initiative. Be clear and specific about your commitment, so that action can easily follow.
- Create an internal culture of equity. Organizational change is rarely easy. Commitments to health equity may challenge current policies, procedures, or status quo. It may take effort to get everyone on board. Without a shared understanding among staff, it may be difficult to move forward and make meaningful change. Create an internal culture of equity by ensuring everyone at the LHD—regardless role—has access to information and education about the differences between equity and equality, the role of social determinants of health, and systemic inequities. This may be a compliment to diversity, equity, and inclusion (DEI) work—not covered in this section—which can drive change of internal practices.
- Build staff capacity to promote health equity. Seek out and provide LHD staff with opportunities for continued education about health disparities and health equity. Continued education may include trainings, personal development opportunities, or cross-department “lunch and learns” that allow staff to hear about equity work happening in other parts of LHD. See the guidance in the Workforce Capacity section to help you look for, vet, and offer trainings in health equity, social determinants of health, and cultural humility.
Use available data- See the Data and Surveillance section for more information about how best to use data. Specifically consider:
- Sources of data related to social determinants of health such as local transportation, education, poverty-levels, housing availability/costs, unemployment rates, and resource/benefit availability can reveal potential factors that contribute to health disparities. By collecting data about the local bus system, for example, you may learn how many people use it, where the bus routes do or don’t go, and their frequency. If bus routes neglect a part of town primarily, this could greatly impact access to services for those inhabitants and lead to negative health outcomes. Root cause indicators, such as the Social Vulnerability Index are another way to identify relevant factors in the community.
- Public health surveillance data, including risk factor surveillance data, mortality surveillance data, and syndromic surveillance data. Consider what this broader data tells you in comparison to local data. For example, if young adults (ages 18-24) make up 25% of the local population and represent 80% of local overdose deaths, this group is likely disproportionally affected.
Learn from the community- Interface directly with community members to gain information about the who and why of local health disparities:
- Conduct or review a needs assessment such as a Community Needs Assessment (CNA), Community Health Assessment (CHA), or Community Health Improvement Plan (CHIP).
- Invite community members to provide direct feedback in a focus group and develop questions that help you gain insights about members’ experiences, perceptions, and opinions.
- Observe trends, such as an increase in community members seeking a particular service, ask partners if they are observing the same trends, and look at available data sources that could corroborate anecdotal information.
Learn through partnerships or collaborations- When possible, create a reciprocal data-sharing relationship. Connect with partners and collaborators to find out the data they are collecting. For example, organizations who receive grant funding are typically required to collect and report program-related data in their reports to funders. . Even if partners aren’t doing formal data collection, consider asking:
- Which of their programs have been most successful and why?
- What has not been successful and why?
- What are they hearing from community members about needs and barriers?
Now that you have identified local health disparities at the intersection of suicide, overdose, and ACEs, focus your efforts on addressing these disparities.
Strive for equity vs equality: Health equity requires efforts to ensure that all people have full and equal access to opportunities that enable them to lead healthy lives.[1] The image below, developed by the Robert Wood Johnson foundation, illustrates the difference between equity and equality.
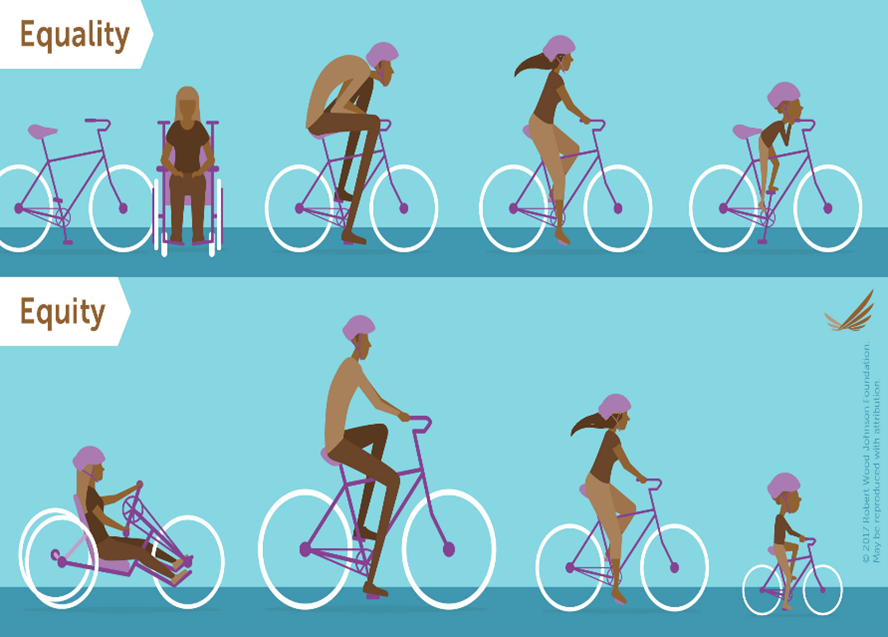
In the same way that each person in this image receives the specific bicycle that works best for them, ensure that services are most likely to benefit people in the community when they are tailored fit groups’ specific needs. This may involve offering more to some groups than for others to achieve the same level of equity. More might equate to more resources, more support, more innovation, more programming. Be unapologetic in those cases where you must offer more to some groups than others to achieve equity.
Be intentional about your efforts from the beginning: Look at the needs and barriers of your disproportionately affected groups and intentionally work to address them from the first step of developing a solution. For example, if you have identified lack of transportation as a barrier to program access, incorporating a transportation solution into the program development may help to remove that barrier. If groups in your community have limited work schedule flexibility (e.g., shift work or hourly work without benefits), offer flexible programming multiple times throughout the day (including evenings) and on weekends. This includes bringing community voices to the table from the beginning so that they can be a part of determining the direction of the programming, rather than waiting until the end when it is too late to make significant changes. One way to do this is by developing a Community Advisory Board (CAB) to participate in discussions and help identify possible solutions. Additionally, avoid launching programs or initiatives that only partly solve the problem, such as limited evening or weekend programs, special transportation that must be applied for ahead of time. Start with the Evidence Based Strategies section [CA 1] for ideas about programming that addresses the intersection of suicide, overdose, and ACEs, and then work with members of your community to decide which strategies should be considered further.
[CA1]Hyperlink to this section
Continue practicing intentionality at every step in the process: Improving health equity is an ongoing process, not a box to simply check off during planning. Consider some of the following strategies to incorporate health equity into all aspects of the work, even once the program has launched:
- Work with your community to determine the types of questions should be asked, and use their guidance and feedback to inform the development of data collection instruments, where possible.
- Make data and needs assessment results available to the community. Include their insights about the meaning of these data. Use the data and insights in strategic planning.
- Provide opportunities for leadership and power sharing to everyone “in the room", particularly members of the community.
- Consider who is not “in the room” and expand opportunities for input and reach.
- Listen to internal and external voices – integrate their perspectives and insights and take action to address the concerns and issues raised in these conversations.
- Always strive for transparent and inclusive communication.
[1] Daniels, G. A. Social determinants of health: The basics. Promoting health equity, a resource to help communities address social determinants of Health.
[2]
Robert Wood Johnson Foundation. (2017). Visualizing health equity: One size does not fit all [infographic]. https://www.rwjf.org/en/librar...
People with lived experience are those who are or have been directly impacted by the issue or topic of focus. People with lived experience in suicide, overdose, and/or ACEs, as well as disproportionally affected community members, are vital contributors in your efforts to address health disparities. LHDs vary greatly as to how much they are engaging the community and in what ways. Your agency may currently be in the early stages, such as eliciting feedback and perspectives from these community members and incorporating what you learn. In this stage, you may incorporate perspectives of those with lived experience:
- As you develop initiatives or programs. Get buy-in and input from the beginning.
- Once a plan, program or policy is in place. Ask the people who will benefit from your plan to tell you where it misses the mark and what they would change.
- As part of a program pilot or soft launch
- As an integrated quality improvement (QI) process
This work doesn’t stop at consultation, however. Even if you are asking the community for their thoughts and ideas, you can begin working toward deeper and more meaningful engagement of those in the community. This involves integrating community needs and assets into processes and planning, ensuring community capacity to play leadership roles, and engaging in community-driven decision-making.
Consider The Spectrum of Community Engagement to Ownership to guide a discussion about where your LHD is in this work.
- If your LHD is already doing work to engage these groups, take time to evaluate those efforts. Where on the spectrum would you place this work? How is it going? What might you need to change?
- If your LHD is not currently engaging these groups, what’s getting in the way? What information, resources, support might your LHD need to begin engaging and incorporating feedback and perspectives from these groups?
Engaging or recruiting people with lived experience must be done appropriately and equitably. Consult the following resources for best practices on how to do so:
-Engaging People with Lived Experience Toolkit
-Engaging People with Lived Experience: A Toolkit for Organizations
See the Multilevel Leadership section for more information and resources on how to engage community members and people with lived experiences.
- Health Equity and Social Justice (NACCHO)—A webpage with information about NACCHO’s Health Equity and Social Justice program including details about the program’s work, training opportunities, resources, policy, and recommended reading.
- Roots of Health Inequity (NACCHO)— An online learning collaborative from NACCHO that provides participants with information on how to explore the social processes that produce health inequities, strategize effective ways to combat these inequities, and work with other local health departments to ensure an emphasis on the incorporation of equity in programming.
- Trauma, Equity, and Resilience (Milken Institute School of Public Health)— A resource repository from the Milken Institute School of Public Health and the Sumner M. Redstone Global Center for Prevention & Wellness that includes information on fostering health equity and building community resilience, including a series of modules designed to highlight the underpinnings of structural racism and to guide conversations about equity.
- THRIVE: Tool for Health & Resilience in Vulnerable Environments (Prevention Institute)— A guideline from the Prevention Institute that can help support health equity and inform programming and policy under this lens.
- Health Equity Guide (Human Impact Partners)— A resource repository from HealthEquityGuide.org that contains categories of strategic practices to advance health equity on the local level.
- Promoting Health Equity: A Resource to Help Communities Address Social Determinants of Health (Centers for Disease Control and Prevention)— A workbook containing frameworks, guidelines, and program descriptions of health equity initiatives in various communities.
- Health Equity (American Public Health Association)— A resource repository that includes health equity fact sheets, briefs, reports, and infographics.
- Engaging Parents and Youths with Lived Experience: Strengthening Collaborative Policy and Practice Initiatives for Families with Mental Health and Substance Use Disorders (National Center on Substance Abuse and Child Welfare)—A resource from that provides key considerations for engaging parents and youth with lived experience in the child welfare and foster care systems.
- Preventing Suicide Requires a Comprehensive Approach (Centers for Disease Control and Prevention) — An infographic and strategic guidelines for preventing suicide in disproportionately affected populations.
- Disparities in Suicide (Centers for Disease Control)— A webpage with facts, resources, and guidelines for addressing disparities in suicide and preventing suicide in those groups disproportionately affected.
- Risk and Protective Factors in Racial/Ethnic Populations in the US (Suicide Prevention Resource Center)— Fact sheets with information about specific protective and risk factors relevant to different racial/ ethnic populations to consider when creating suicide prevention programming.
- Suicide Prevention Modules: Module 3: Bringing equity to suicide prevention (Prevention Institute) —A module focused on creating equitable suicide prevention programs.
- Health Equity in Response to Drug Overdose (NACCHO)— A resource repository from NACCHO providing a variety of actionable and supplemental resources on health equity in drug overdose prevention and response.
- Strategies to Address the Opioid Epidemic in Black and Hispanic/Latinx Communities (National Network to Eliminate Disparities in Behavioral Health)— A webinar series and supplementary resources from the Substance Abuse and Mental Health Services Administration Office of Behavioral Health Equity that provides an overview of the opioid epidemic in minority communities. The webinar also provides strategies to decrease the proportion of Black and Latinx populations dealing with substance use disorders.
- Training and Educating Public Safety to Prevent Overdose Among Black, Indigenous, and People of Color Communities (National Council for Mental Wellbeing)-A report from an environmental scan conducted to help create key findings regarding BIPOC communities and their experiences with overdose and public safety.
- Integrating Health Equity into Overdose Prevention and Response: An Environmental Scan (NACCHO)- A resource designed to identify existing barriers and facilitators local and state health departments face to advancing health equity in their overdose prevention or response efforts.
- Medication-Assisted Treatment for Opioid Use Disorder in Jails and Prisons (Vital Strategies and National Council for Behavioral Health)—A toolkit from the National Council for Behavioral Health that contains information to advance the implementation of evidence-based medications for opioid use disorder within jail and prison settings.
- Racism and Discrimination as Risk Factors for Toxic Stress (ACEs Aware)- A webinar about the intersection between health equity and ACEs. Specifically, the webinar discusses how exposure to racism and discrimination are risk factors for toxic stress.
- Exploring the Rural Context for Adverse Childhood Experiences (ACEs) (National Advisory Committee on Health and Human Services)- A report that includes a policy brief and recommendations for preventing and addressing ACEs in rural areas.
- Preventing Adverse Childhood Experiences: Leveraging the Best Available Evidence (Centers for Disease Control and Prevention)— A report that contains information on evidence-based ACE prevention practices.
This page is part of the SPACECAT Toolkit. It was last updated on September 22, 2022. To report broken links, please email [email protected].